DOCUMENTATION/ PAPERWORK
I will be honest. I always have difficulty with this one. With the experience of working at different agencies, I would say I am not 100 percent expert but was able to be better at writing my notes. Each and every agency have its own way of documenting notes. But these are my favorite way of doing it.
Treatment Plan- My favorite find
Whoever created this pdf, they are a godsend for me. Luckily, after I created this website. I received an email via LinkedIn from the creator Kimberly Fore. She created this cheat sheet for the therapists she supervised. She also said she is happy that it has been helpful and also welcomed me sharing it with you guys. This 11-page pdf has specific examples of goals, objectives, and interventions for different topics (abuse/ neglect, addiction, adoption, anger, anxiety, behavior problems,…..and the list goes on). I lost my pdf after I left one of the jobs, and am so glad I found it again. https://studylib.net/doc/7892034/treatment-plan-goals-and-objectives
PROGRESS NOTES
Usually, I am famous for writing too much. However, these are the bullet points I usually focus on.
-
- Progress on goals: This is straightforward. Since the last session, how did the patient do? Were they able to achieve the goal/ did worse?
- Engagement: This is where I write the patient’s engagement. Usually, it is super easy to write up “Patient was engaged and involved in the session”. or “Patient was refusing to participate, defiant, disrespectful, noncompliant, or aggressive”.
- Interventions used by the provider: I just make it basic giving little detail on the interventions “improve or teaching skills”, “explore and process”, and specific modalities “CBT, DBT, play therapy, family therapy….”.
- Reactions/ Interactions by the patient: I am not even sure if I should be giving recommendations on this one. I give too many details myself. Hehehe. But I use this one to remind myself of any basic bullet points that I can use later in the sessions”their stress, triggers, belief system, and their reaction to homework given/ interventions suggested”.
SOAP Notes
positivepsychology.com has a pdf that you can use to write your notes. It uses S= Subjective, O= Objective, A= Assessment, and P= plan. You can find the pdf and also read more on how to write notes. https://positivepsychology.com/soap-notes-counseling/
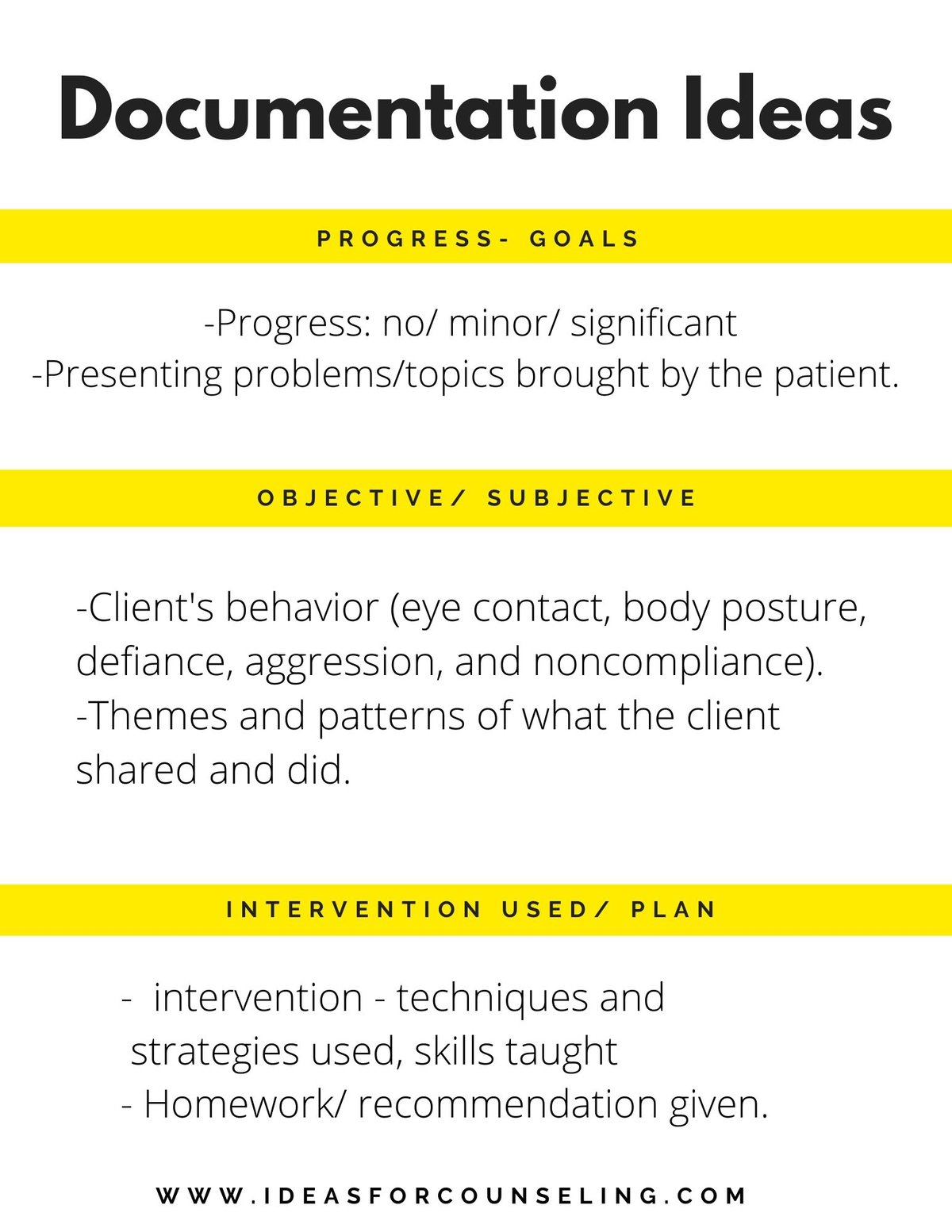
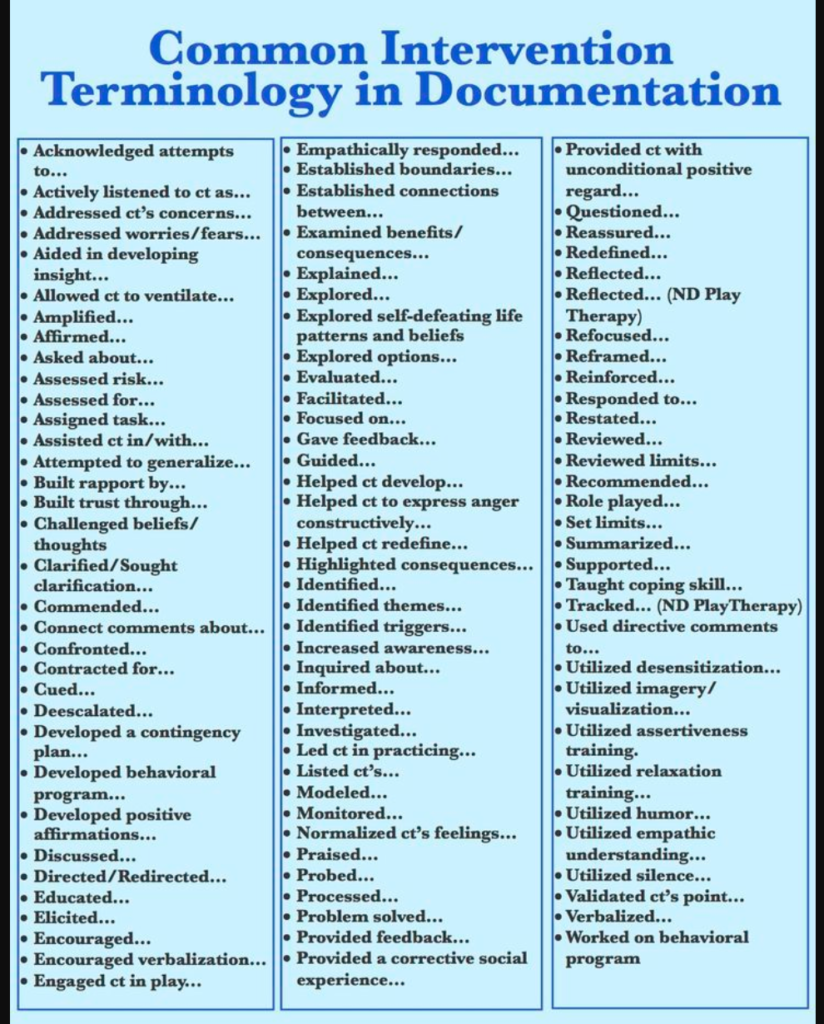
INTERVENTION TERMINOLOGY
I am not sure if you have seen this one online. But this one is a famous one too. It lists common intervention terminology in the documentation. I am not sure who created this. But these words help a lot when I am writing my documentation. https://www.pinterest.com/pin/534169205775458559/
SAID SYNONYM
I don’t know about you. But I also have a very difficult time finding other words than said, when I am doing my paperwork. If that’s you. Here is a list of words you can use other than said.